
Group discussion between Local Village Health Volunteers as part of a BHCP orientation exercise in the Bana District in 2014 (Credit: BHCP)
Integrating formal and informal institutions: towards a healthy community in Bougainville
By Lhawang Ugyel
19 July 2018
The case of the Bougainville Healthy Communities Program (BHCP) stands as a testament of how an organisation can work effectively in PNG in delivering critical services. BHCP started as an off-shoot of the successful implementation of the leprosy elimination program in Bougainville funded by the New Zealand government in 2001. Following the success of the leprosy program, a new project proposal was submitted to New Zealand Aid to promote health awareness. In 2006 the program was rolled out in three of the 13 districts in Bougainville, with a small group of staff that included the program manager and three district facilitators.
An evaluation of the BHCP was commissioned by the New Zealand Ministry of Foreign Affairs and Trade in 2012. The evaluation found that the BHCP is an ‘excellent example of a well-planned and well-executed public health and community development model… implemented within the enormous constraints and challenges of a post-conflict setting’. In the July 2016 half-yearly summary report, various indicators reflect its effectiveness in promoting health awareness and educating people in basic health care. Figure 1 shows the increase in referrals since 2014, particularly in TB, malaria and number of births, and that an area that the program needs to focus on is sanitation.
Figure 1: Outcomes of the BHCP

*Proportion (in percent) against total suspects made by Village Health Volunteers; **proportion (in percent) of babies born; ***proportion (in percent) of families
Source: ABG DOH, 2016
At a time when PNG, and particularly Bougainville, faces multiple political and socio-economic challenges, the success of BHCP gives some hope. To understand the reasons behind its success, I conducted research into the program, including interviews with key people involved with the BHCP. Findings of the research highlighted some key factors attributing to BHCP’s success: generous and sustained donor support; good leaders; a committed group of people working towards a common goal; and, unique to BHCP, the integration of formal and informal institutions in the delivery of public health services.
The integration of institutions is important, and the ‘right mix’ of institutions is visible in the case of BHCP. Douglass C. North provides the most common definition of institutions: that they are the humanly-devised constraints that structure political, economic and social interaction. This definition encompasses aspects of both formal and informal institutions as a combination of formal constraints, informal rules, and their enforcement characteristics. In practice, the focus is mostly on the formal institutions, but the role of both formal and informal institutions is important. Such mixes of institutions are particularly important in countries where local government plays an important role in the provision of local services and infrastructure, but there is also a risk that these governments are over-tasked, which affects performance.
Figure 2 below shows the structure of BHCP, and how it relates to government. The figure is divided into four main quadrants. The government and the non-governmental systems form the horizontal rows, and formal and informal systems the vertical columns. Section 16(35) of Bougainville’s Constitution provides for partnerships in the provision of health services. At the local government level is the community government (earlier the council of elders) that is comprised of leaders from the village assemblies. Based on the definition of formal institutions where structures are legally organised, the government departments and the community government form the formal system in Bougainville. The informal system in Bougainville includes the village assemblies, which are supported by the village authorities.
Figure 2: Structure of the BHCP within the overall system of governance
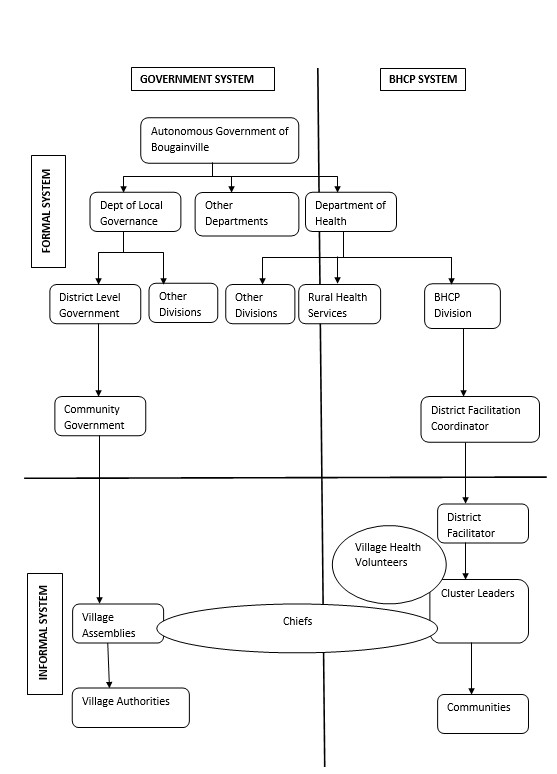
Currently, BHCP functions as a non-governmental program. The BHCP program manager and the two district facilitation coordinators are paid by the government. Under the district coordination facilitators are the district facilitators. These district facilitators operate at the informal level and liaise directly with the leaders and chiefs of the villages. Each village also has one to two village health volunteers, who are the point of contacts for the district facilitators. The village health volunteers and district facilitators while working for the BHCP play an important role as a link connecting the people to the formal health system.
In a typical setting, informal and formal institutions are seen as operating independently, and often formal institutions are given preference over informal ones. As the notion of government as a single decision making authority has widened to include multiple actors, the divide between formal and informal institutions and actors begins to blur. The overlap between formal and informal institutions are sometimes necessary to lead to positive outcomes. The manner in which BHCP functions is an example of an integration between its formal and informal institutions. All actors within the four quadrants play an equally important role in implementing the activities of the BHCP.
The lessons from BHCP’s experience should be used to allay concerns of the lack of capability in PNG for effective service delivery mechanisms. While challenges certainly remain in their formal institutions, the governments and NGOs of Bougainville and PNG should look to the strength in their informal institutions to work together in improving governance.
Read the full paper here.
About the author/s
Lhawang Ugyel
Dr Lhawang Ugyel is a lecturer at the School of Business, University of
New South Wales, Canberra.
