

Papua New Guinea (PNG)’s low COVID-19 vaccination rate is well known. This blog provides some context for that, and points to the wider problem of falling national immunisation rates.
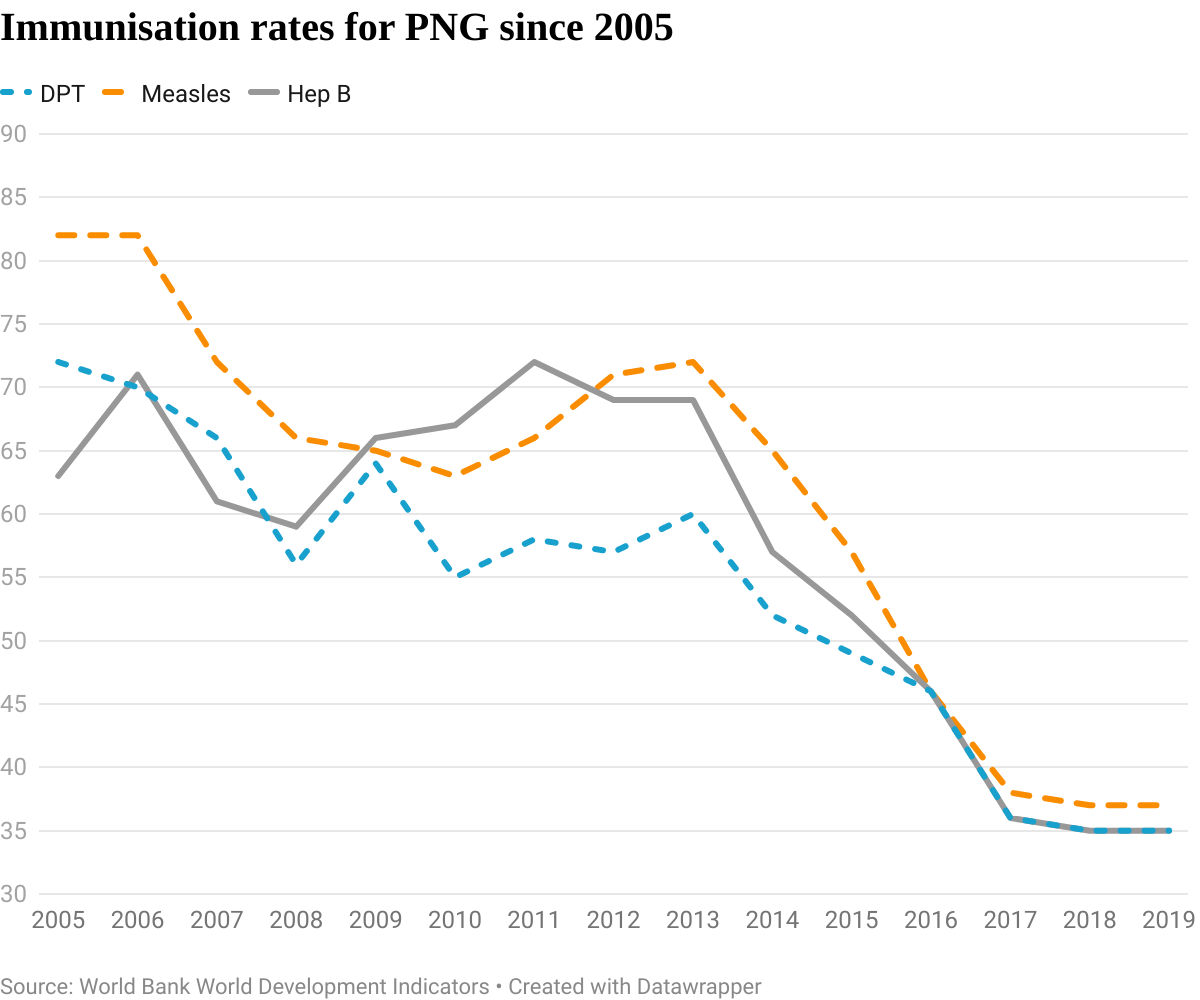
The World Bank reports data immunisation coverage for nearly all countries in relation to three vaccines: the measles vaccine; the combined vaccine for diphtheria, whooping cough and tetanus (DPT); and the hepatitis B vaccine. On all three, the most recent data (for 2019) show that PNG has the lowest vaccination rates in the world for infants: 37% for measles, 35% for DPT and 35% for hepatitis B.
PNG has been a bottom-ten immuniser for measles and hepatitis B since about 2015, and for DPT since about 2010. It has been the worst or second worst immuniser for all three since 2017.
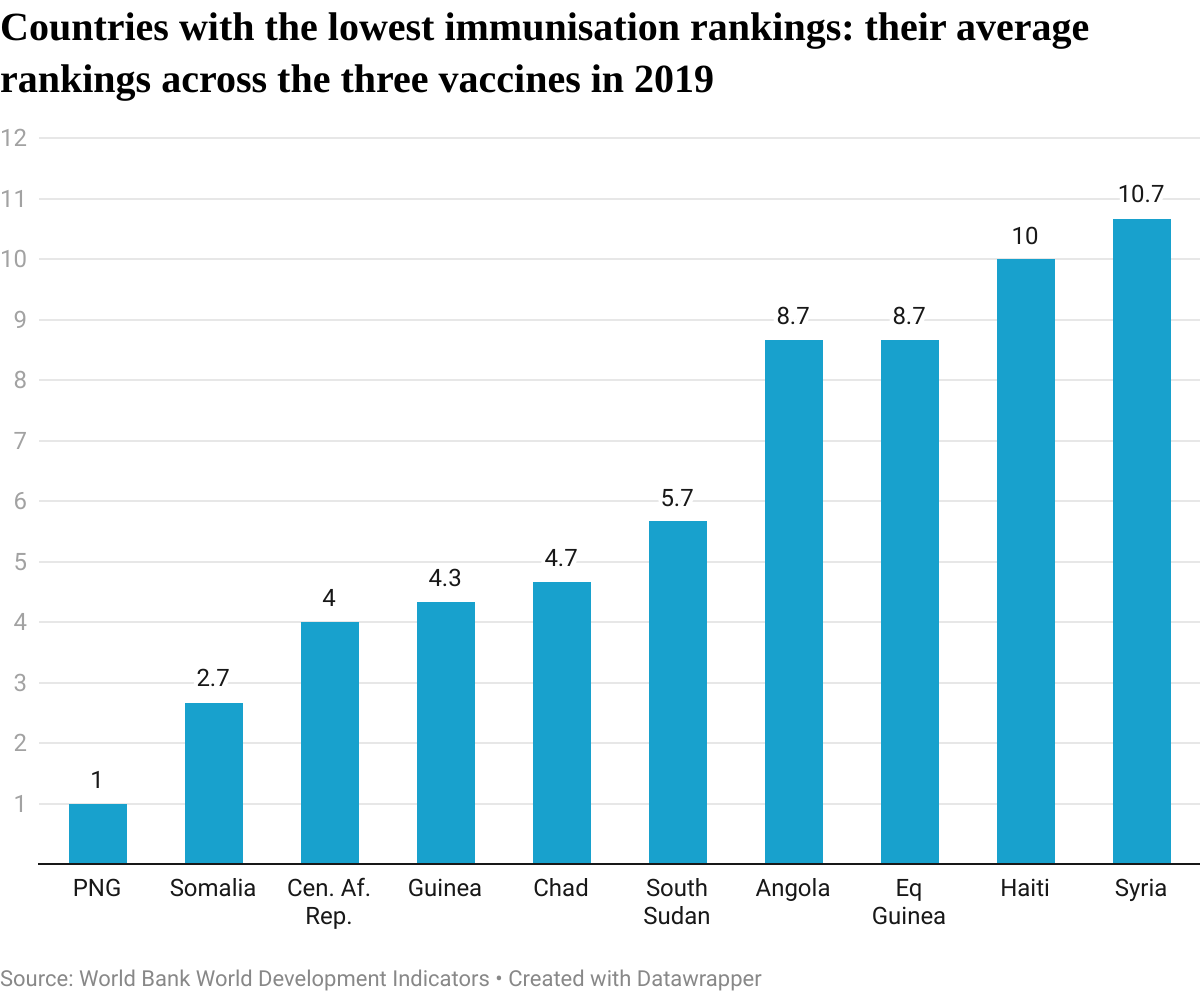
The graph below shows the average ranking across the three vaccines for the ten countries which have the lowest rankings on average for 2019. It is generally a group of countries facing crises of terrorism, refugees and/or large-scale conflict. Plus PNG.
How to explain this shocking fact?
Explanations based on PNG’s characteristics struggle in the face of comparisons across countries. We might say PNG is a fragile and conflict-affected state. The average for fragile and conflict-affected states is 67% for both DPT and measles, and 68% for hepatitis B. We might say that service delivery in Melanesian countries is generally poor. Immunisation rates in Vanuatu and Solomon Islands are 80% or higher for measles, and 90% or higher for DPT and hepatitis B.
A standard explanation is that PNG is geographically challenging, populated by hard-to-reach, remote communities. But that doesn’t explain why PNG’s vaccination rates have plummeted over the last 15 years.
Perhaps the data is wrong. 2019 was in fact meant to be PNG’s ‘year of immunisation’, the year in which, responding to an outbreak of polio, a massive immunisation drive was conducted, with significant donor support. According to UNICEF, more than a million children were vaccinated against measles (as well as rubella and polio) in a nationwide campaign that year. But the World Bank data (which comes from UNICEF and the WHO) tells a different story. So does PNG’s own national data (presumably the original source), which puts measles vaccination rates in 2019 at 34%, and the combined DPT/hepatitis B vaccine at 42%. These numbers show no improvement at all over previous years, simply a halt in the deterioration.
Perhaps then there are problems with the quality of the PNG immunisation data (and more generally PNG’s over-elaborate health data collection system). The comments in the UNICEF/WHO country report hint at this. But, even if there are question marks around PNG’s precise immunisation rate, the country’s own national program and survey data both confirm the collapse in PNG’s immunisation rates over the last 15 years or so.
Immunisation rates improved over the 1990s. The real collapse in rates came between 2013 and 2017.
The emphasis then was on providing funds for MPs to spend on local projects. None of this went on health service delivery. There was a famous drug corruption scandal. The resource boom was over, and revenue was falling. Health budgets were cut (after inflation, by 9% between 2013 and 2017). Then Prime Minister Peter O’Neill introduced a ‘free health care’ policy at the start of 2014. Health facilities were discouraged from charging user fees, their most reliable source of revenue. Analysts warned at the time that this would weaken the health system.
Meanwhile, Australia was reorienting its aid to PNG over this period away from service delivery!
Whatever the questions around the accuracy of PNG’s immunisation data, there is plenty of evidence that immunisation rates had deteriorated to crisis levels prior to COVID-19. Controversies over the COVID-19 vaccine will only make the general immunisation task that much harder. We can debate whether PNG is a failed state. But this is a clear case where the state has failed its people.
Data from World Bank World Development Indicators. Measles and DPT coverages are reported in relation to two year olds; hepatitis B in relation to one year olds. The DPT and hepatitis B vaccines are now combined in PNG so the two series have converged. Health budget data from WHO.

Disclosure
This research was undertaken with the support of the ANU-UPNG Partnership, an initiative of the PNG-Australia Partnership. The views represent those of the authors only.
This is an important article. It captures the major decline in the national health budget between 2013-2017, which dealt an almost fatal blow to primary health services.
But this is not the only factor driving these alarming statistics. Since the 1980s the primary health system has progressively lost its ability to undertake outreach and connect with the communities it is supposed to serve. Once a staple of primary health services, immunisation and antenatal outreach is essential if population coverage is to be achieved.
The figures quoted from the Solomon Islands are instructive. While a much smaller country, nonetheless the geography can be equally as challenging. I remember carrying a cold chain box up a mountain side on Isabel island in 1980 as a volunteer mule for a health team on immunisation patrol. From the statistics presented in this article I gain the impression little has changed there.
By comparison, in PNG you would struggle to find a community health worker who regularly sets out on foot to visit communities on the hill, or the next valley. They generally run an aid post clinic walk in service that may, or more typically may not have cold chain and doesn’t offer vaccinations.
This leaves the practice of the annual (if you are very lucky) immunisation drive undertaken by NGOs in collaboration with provincial health workers. In short, the process is hugely underfunded, piecemeal, incomplete and nearly always reliant upon NGO participation.
What characterises this approach is the service is not owned in any sense by those who need it, and it is never sustainable.
For example, a look at the geography of Milne Bay or Southern Highlands provinces should tell a planner, logistician or health worker that service delivery by government alone is out of the question.
In the 1980s Milne Bay communities located on the remotest islands were served by a fleet of government ship-based health centres. In the mid 1980s the World Bank financed a multi-sectoral rural development project in the Southern Highlands that included transport to deliver health workers to remote sites. Today both initiatives are long gone.
Both approaches represented the bold idea that with adequate funding and commitment, government would support these strategies into the future. This thinking still prevails and in the face of half a century of failure, it is plainly wrong.
No amount of public sector strengthening will solve these issues as ongoing efforts will discover. In short, “government” in the image of a Westminster system does not represent “the people.” Only a deep dive into the traditional views that underpin community culture and politics will explain why this will remain the case.
In my view, as a first-hand observer, I believe the solutions, if any, lie in placing the onus for supporting the delivery of services to communities where it has always belonged – with the communities themselves.
They are the ones that can solve the issues around transport, access to where they live, construction and maintenance of infrastructure and guarantee health and education workers and community policemen a safe working environment. Not government.
I am prepared to bet that if an area of Milne Bay that does not receive services was thrown the challenge, that as a pre-requisite the communities must provide safe transport, maintain infrastructure and whatever else to ensure immunisation and antenatal services reach them regularly. And that henceforth the services they receive would be dependent upon their contribution, they would do it.
There is a PNG civil society driven initiative to do this, but because it is not wholly under the umbrella of government it is not funded. Given the track record since independence, reflected so grimly by the immunisation statistics reported in this article, I would urge development assistance planners to step outside the square and try something different.
I believe that health indicators are arguably some of the best indicators of good governance and development of a country. The plummeting immunization rates is a red flag signaling a failing health system and a failing government that is unable to deliver basic services.
We are now faced with a double burden of diseases – prevalent infectious diseases and the rising non-communicable diseases!
Much of the talk these days among government leaders is about building super hospitals and sophisticated equipment but fail to recognize that we have a primary health care that is in a mess. There is more that needs to be done within the space of primary health care – the basics!
A worrying set of findings for several reasons. First, immunisation against those and similar diseases are effective in preventing death and disability especially among the poor. UNICEF, for example, estimates that vaccines save five lives every minute globally, and prevent up to 3 million deaths a year.
Second, vaccination programs are very affordable and cost-effective in the vast majority of countries and circumstances worldwide.
Third, and interestingly, a political-economy side-benefit of vaccination programs is that they demonstrate a government can provide essential services even to remote areas, increasing the visibility of governments and, potentially, even the political “legitimacy” of governments.
Finally, if governments like PNG struggle to deliver and maintain basic and essential immunisation programs such as measles, DPT and Hep B, it does raise the question as to how well they can then respond to the usually much more expensive and complex challenge of responding to non-communicable diseases such as diabetes, heart disease and stroke. That is relevant to PNG because the Institute of Health Metrics and Evaluationestimates that diabetes, ischemic heart disease, and stroke are now in the top five causes of death in PNG, showing a 51.4%, 45.2% and 36.6% increase respectively over the 10 year period 2009-2019