

Many people think tuberculosis (TB) is an ancient scourge that has already been defeated, yet in reality it remains the world’s leading infectious killer despite being curable. Scientific advances mean ending TB is more achievable than ever, but too many people with TB are still missed.
An uncomfortable and mostly unspoken reason for this is that active case-finding — long appreciated as the best way to eliminate TB — has long been considered too hard and too expensive for people in high-transmission, lower income settings. On the back of technological advances, this can change.
Current approaches rely heavily on people presenting to health facilities and being able to cough up a sputum sample for testing. In practice, many people with TB have few or no symptoms, or face barriers to accessing care. As a result, transmission continues undetected. In high burden areas, symptom-based TB control is simply not enough.
This is where policy and investment choices matter. If we are serious about eliminating TB, we need to shift from facility-based models to approaches that actively identify people with TB in the community regardless of their symptoms so they can rapidly receive treatment and stop the transmission cycle.
Population-level screening has proven to be successful in eliminating TB in some settings.
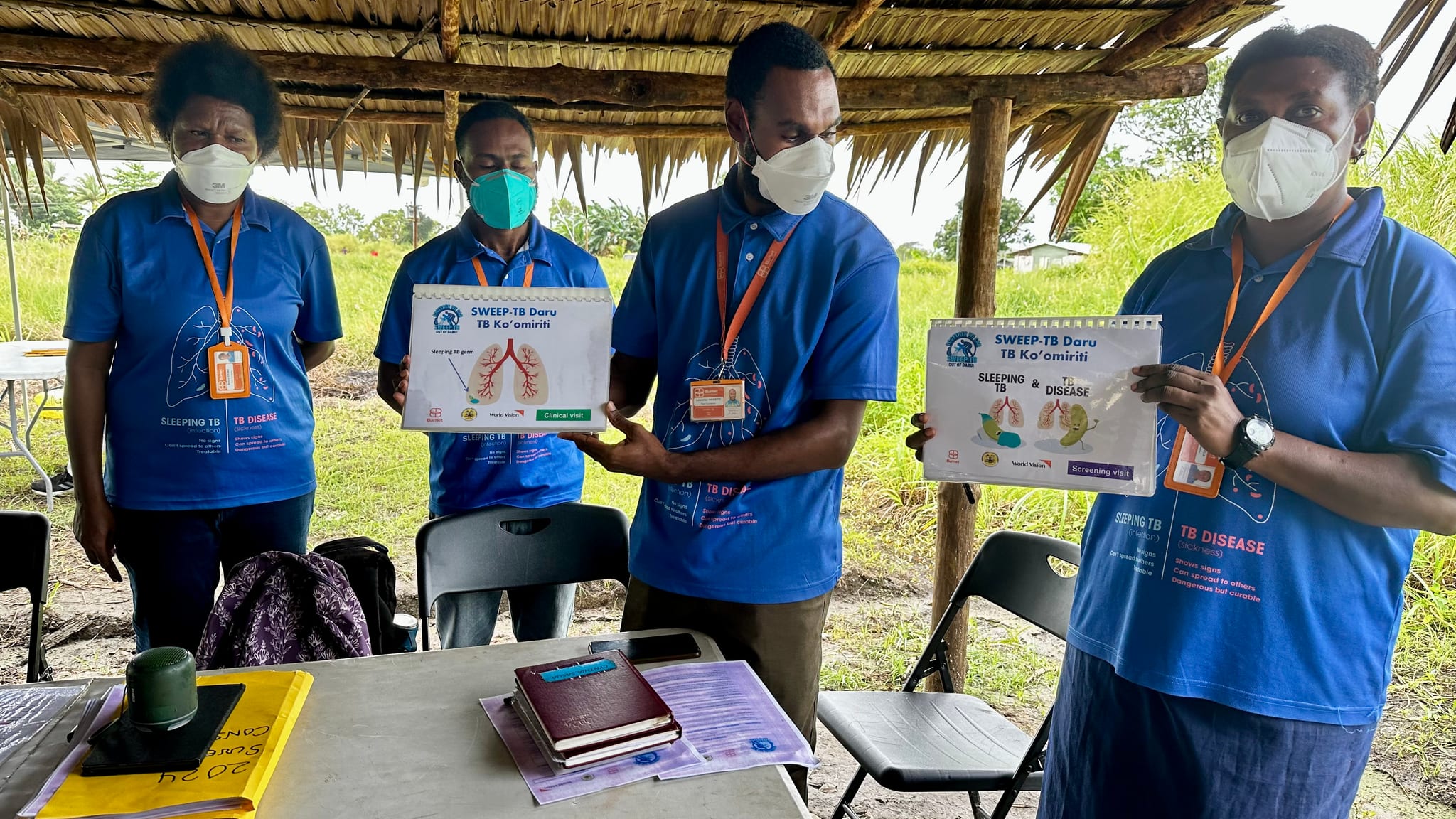
In Papua New Guinea, where the TB burden remains high and access to timely diagnosis is uneven, Burnet Institute has been working with partners on Daru Island in the country’s Western Province, a recognised hotspot for multidrug-resistant tuberculosis.
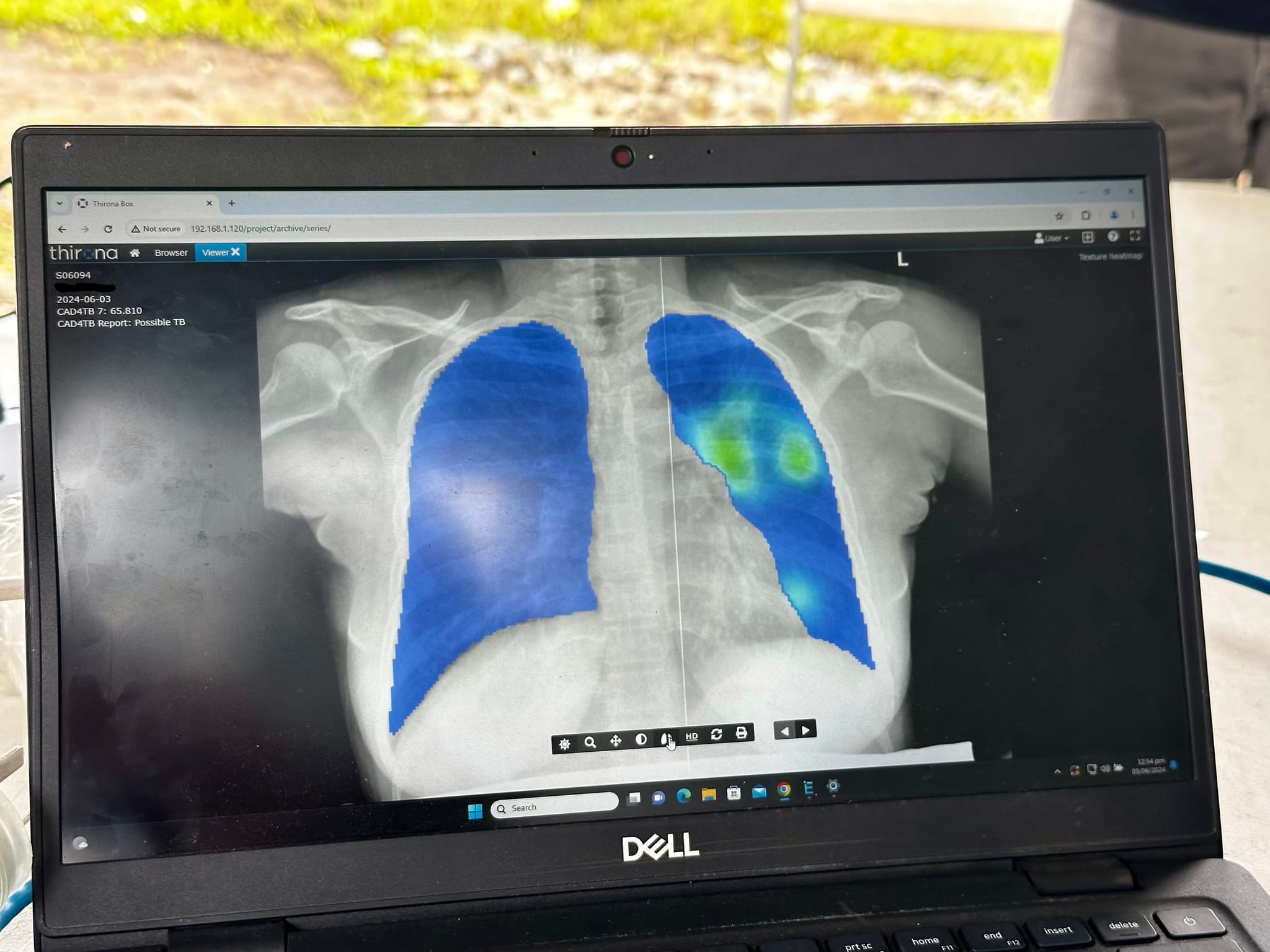
The approach is simple: test everyone and provide treatment for anyone who has TB. By combining community engagement with active case finding, including mobile digital X-ray, this model has identified many previously undiagnosed people with TB and shown what’s possible when screening moves out of healthcare facilities.
Ongoing work in East New Britain province has shown the value of expanding ways of testing for TB by bringing services directly to people’s workplaces and testing for related conditions such as diabetes and hypertension.
While this model works, it is not easily scalable. Mobile X-ray units and screening buses are costly, complex and difficult to deploy in remote areas. Expanding TB detection will require simpler, more adaptable tools.
A new approach recently endorsed by the World Health Organization uses a tongue swab instead of sputum. Many people cannot produce sputum, including children, people living with HIV and people in early stages of TB disease. A tongue swab is non-invasive and easier to use in community settings.
This portable tool is battery-operated and relatively low cost and will be piloted in collaboration with Burnet and the PNG Government in everyday settings such as local transport hubs, markets and village centres, as well as in-home screenings.
Advances in portable digital X-ray, supported by artificial intelligence for rapid interpretation, have been improving large-scale screening for more than a decade. These tools are most effective when combined with community-based approaches that engage local health workers and leaders.
There are also critical gaps in how TB is detected and managed in specific groups. Pregnant women are often overlooked — the burden of TB in pregnancy is higher than in non-pregnant women, and diagnosis is difficult. Symptoms may be absent, making symptom-based screening unreliable. Existing diagnostics may also be less sensitive, and chest X-rays are not always appropriate.
Addressing this requires integrating TB screening into routine antenatal care. We’re exploring approaches such as digital stethoscopes combined with artificial intelligence to identify women at risk in a safe and non-invasive way. This kind of integration is essential if we are to improve detection without adding new barriers to care.
Better tools are also needed to monitor treatment response for people receiving TB treatment. Currently, there is no simple way to assess whether a patient is responding well before their condition worsens. Developing a test that combines laboratory and clinical data to provide early insight into treatment response would allow care to be adjusted sooner and improve outcomes.
Ending TB will not come from a single breakthrough. It will require sustained investment in practical, scalable solutions that make detection faster and more accessible for everyone. It will require a mindset shift for policymakers: active case finding is a must no matter what the setting.
On this World TB Day, the priority should be clear. We must back approaches that bring diagnosis closer to communities, invest in tools that are simple to use at scale and ensure that no one is excluded because current systems are inaccessible. With the right policy choices, eliminating TB everywhere, not just in wealthier jurisdictions, is within reach.





