

The first article in this series reported on the latest trends in development assistance for health and the second focused on the rise of non-communicable diseases (NCDs) globally and especially in low- and middle-income countries. This final article provides recent insights into trends in diabetes, a particular challenge in the Pacific.
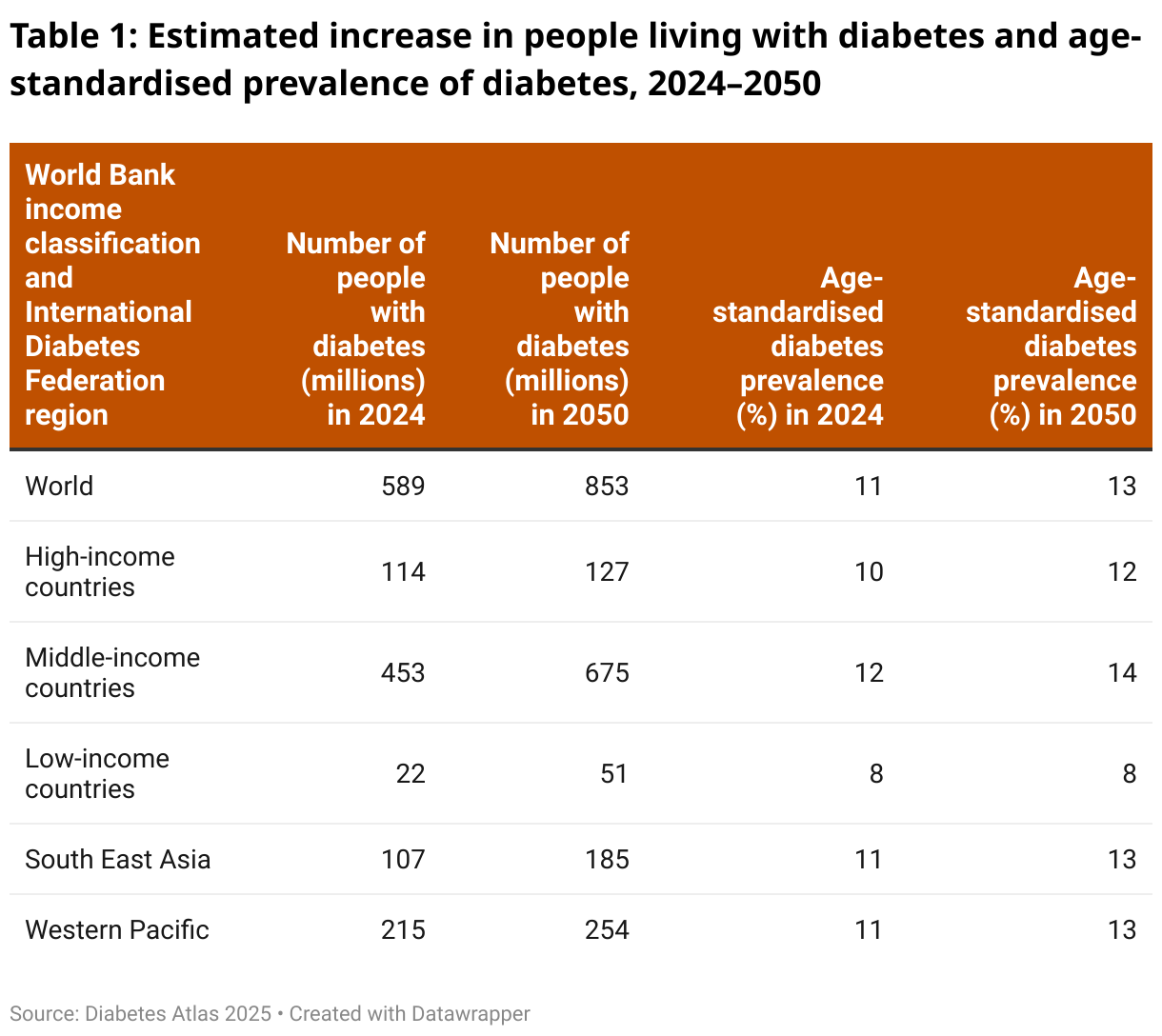
The Diabetes Atlas 2025, recently released by the International Diabetes Federation, presents some new and important analysis global and regional trends for diabetes. It concludes (page 95) that “if left unchecked, the current global prevalence of diabetes at 589 million and the anticipated increase to 853 million by 2050 presents a monumental challenge to global health”(Table 1).
The Atlas presents some challenging findings for countries in Asia and the Pacific. It finds that in 2024 five of the top ten countries and territories in the world for age standardised diabetes-prevalence were in Asia or the Pacific (page 48), specifically: Pakistan, Marshall Islands, Samoa, Kiribati and French Polynesia — ranked first, second, fourth, sixth and eighth respectively. It estimates that by 2050 those worrying rankings will be largely the same, although Kiribati will have the third-highest prevalence in the world, Samoa will fall to fifth-highest and French Polynesia to tenth-highest.
An associated challenge in planning for and responding to the growth of diabetes is the currently high level of undiagnosed diabetes. The Atlas estimates that 251 million people globally — or almost half (42.7%) of adults living with diabetes — were undiagnosed in 2024. It finds that in the World Health Organization’s Western Pacific region, which includes all the Pacific Island countries, 50% of diabetes cases are undiagnosed — the second-highest rate of all regions globally.
It reports that the proportion of undiagnosed diabetes cases in people aged 20-79 years in Samoa, Solomon Islands and Timor-Leste was 83.9%, 80.6% and 77.5% respectively. Almost three-quarters of diabetes cases were undiagnosed in Federated States of Micronesia, Indonesia, PNG, Tonga, Vanuatu and Nepal. Eight Asia-Pacific countries had rates of 50% or more of undiagnosed diabetes: Cambodia, the Democratic People’s Republic of Korea, Kiribati, Malaysia, Marshall Islands, Niue, Palau and the Philippines. Vietnam had one of the lowest rates of undiagnosed diabetes in Asia and the Pacific but even then, more than a third (37.8%) were undiagnosed.
The Atlas also explains why diabetes can have such a damaging effect on public health, wellbeing and economic development. Diabetes can directly lead to amputations, as well as sight impairment and diabetic-related blindness. The Atlas also notes how diabetes can interact with and exacerbate other important health challenges. It notes, for example (page 89), that “people with type 2 diabetes are at higher risk of cardiovascular diseases, including a 72% higher risk of heart attack, a 52% higher risk of stroke, and an 84% higher risk of heart failure. … [People with diabetes also have] a 56% higher risk of dementia compared with people who do not have diabetes”.
Not surprisingly, diabetes imposes significant costs on health systems and individuals. The Atlas reports (pages 7 and 41) that “direct health expenditure due to diabetes surpassed one trillion US dollars for the first time and will continue to rise over coming years … this represents 12% of global health expenditure”. It reports (page 2) that total diabetes-related health expenditure in the Western Pacific region was US$246 billion in 2024, second only to expenditure in North America and higher than that in Europe. It finds that diabetes related expenditure per adult was on average US$1,174 in the Western Pacific region in 2024.
Tables at the back of the Atlas report give estimated expenditure on diabetes per person for every country in Asia and the Pacific. An earlier but important article published in 2015 found that annual expenditure on diabetes was approximately 20% of governments’ annual expenditure on health care in Solomon Islands and Nauru. That article also found that indirect costs including work absenteeism, as well as costs of carers — often female — taking diabetic patients for overnight treatment at tertiary facilities, were significant.
To conclude, these three articles — on the decline in development assistance funding for health globally, on the rise of NCDs and on the particular challenges of diabetes — all point to one conclusion. Health outcomes and health financing are not “just” a health issue but important in their own right. They are also an important — and often growing — international development issue.


