

For months, the mpox epidemic has been sweeping through the Democratic Republic of Congo (DRC), with more than 20,000 suspected and confirmed cases, and over 630 deaths recorded from January to early September. On 14 August 2024, the World Health Organization’s Director-General, Tedros Adhanom Ghebreyesus, declared that this surge of mpox cases in DRC and a growing number of other African countries constitutes a public health emergency of international concern. The emergency declaration followed advice from an expert committee warning that the disease has the potential to spread further across the continent and possibly beyond its borders.
In Goma recently, many people I talked to seemed to sense that something new, uncertain, and frightening is coming. But no one can yet predict what it will mean for them or how deeply it will affect their lives.
Mpox, originally known as monkeypox, is not new in the DRC. This contagious viral disease is endemic in the northwest and central provinces, where it mainly affects people who have been in direct contact with infected squirrels. Common symptoms of mpox include skin lesions, fever, headache, muscle aches, exhaustion, and swollen lymph nodes. Most people who are infected recover from their symptoms within four weeks of medical support.
Over the years, outbreaks have been sporadic and limited to certain areas. However, the number of cases has surged over the past two years, with more people affected not only in the traditional endemic areas but also in new areas in eastern DRC, such as South Kivu and North Kivu.
In these regions, a new strain of the virus, known as “clade Ib”, has been identified. While the lethality of clade Ib appears to be significantly lower than that of the strain affecting people in traditional endemic areas, it seems to be more easily transmissible between humans without contact with affected animals. This has led to a faster spread of the disease among people. A similar phenomenon occurred some years ago in Nigeria, where a new form of the endemic clade II also emerged (known as ‘clade IIb’), leading to increased transmission and the global outbreak in 2022.
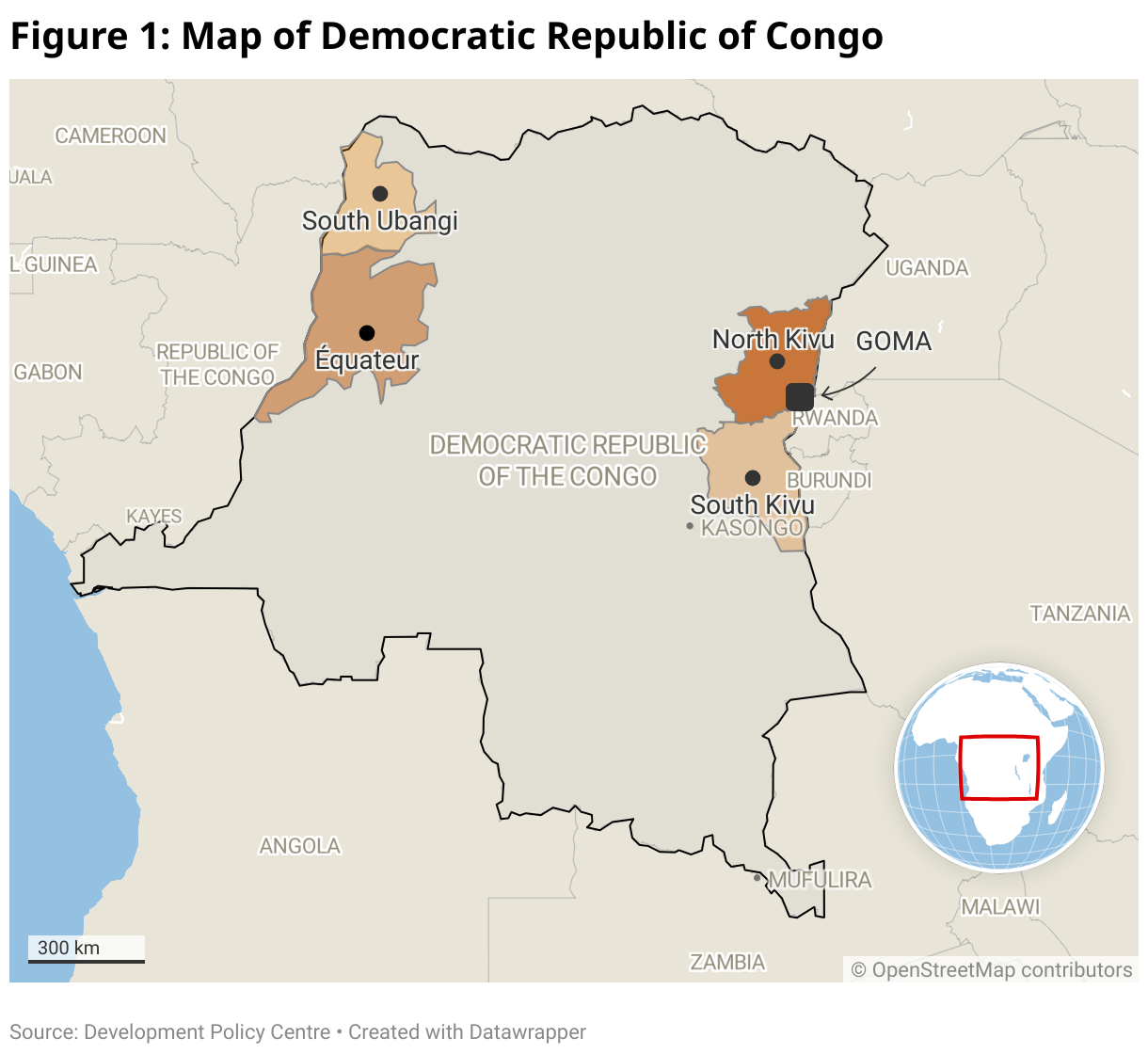
But the situation in DRC is concerning, particularly because cases have been reported in densely populated areas like Goma, a city of two million people, as well as in surrounding sites, where hundreds of thousands have sought refuge from the ongoing armed conflict in North Kivu. The conditions required to prevent the spread of mpox in and around Goma are simply not in place, and the capacity to provide care for patients most at risk of complications – such as young children or people with weakened immune systems – remains very limited.
How can we expect families living in tiny shelters, without adequate water, sanitation facilities, or even soap, to implement preventive measures? How can malnourished children have the strength to ward off complications? And how can we expect this new variant – which is notably transmitted through sexual contact – not to spread in displacement sites given the dramatic levels of sexual violence and exploitation affecting girls and women living there?

Médecins Sans Frontières (MSF) has repeatedly denounced the inhumane living conditions that people face in the displacement sites, and the glaring gaps in the humanitarian response. More than two years since the start of the massive displacements linked to conflict between the M23 armed group and the Congolese army, supported by non-state armed groups, families living in the overcrowded camps still lack basic essentials: food, water, safety, hygiene items, as well as access to sanitation and healthcare.
During a counselling session that I attended with survivors of rape, a woman told me she lives with her seven children under a plastic sheet. Her partner abandoned her after the rape. For women like her, the tried-and-tested solutions to prevent the spread of the epidemic are unimaginably difficult to implement. If she develops a rash due to mpox, she will be told to change her linens, wash everything thoroughly, disinfect her belongings, and isolate herself until she heals. But how can she wash without soap and with only a few litres of water available each day? How can she isolate herself and protect her children while living together under their minuscule plastic sheeting shelter? If she isolates, who will get food for the children? Who will collect firewood? Who will comfort the newborn?
For her and the many others who have sought refuge in the displacement camps, the mpox epidemic feels like just another challenge amid a torrent of problems. And, frankly speaking, mpox is not even the most pressing concern given the daily struggles they face, including other life-threatening diseases such as measles, malaria and cholera.
Yet, mpox remains a threat that must be tackled. To confront this additional challenge, we need to make survival easier for those displaced by violence through a response that is tailored to their specific needs and real-life challenges. This begins with listening to people, understanding their needs, and providing them with essential supplies for infection control: water, soap, disinfectant, proper sanitary facilities. These simple yet vital measures are crucial. Relying solely on the arrival of vaccines won’t solve the problem; improving living conditions is also a critical factor in fighting such outbreaks.
Together with health authorities, our teams do their best to care for patients and raise awareness for those living on the sites, just as we do in other parts of the country affected by the outbreak. Since June, MSF has set up several emergency operations to address the mpox epidemic in four provinces of the DRC (North and South Kivu, South Ubangi, and Equateur) as well as in neighbouring Burundi. These support the prevention and treatment of mpox, awareness raising, and infection control. Like many others, we hope that the long-awaited vaccines, which are now arriving in the country, will rapidly be dispatched to affected areas to protect those most at risk, including patients’ families, to curb the spread of this outbreak and save people from potentially fatal complications.
But vaccines will not be a magic bullet: for mpox, as with other viral diseases, both government and non-government actors must urgently address the factors that contribute to the spread of disease. This begins with listening to people’s needs and adapting responses accordingly. Mpox is just one of the many challenges people face in eastern DRC. The effort to combat this new outbreak should be made, but should not overshadow or negatively affect the response to other critical issues in this region.
This blog is published as part of a partnership between the Development Policy Centre and Médecins Sans Frontières / Doctors Without Borders (MSF) Australia. It is an edited version of a blog previously published on MSF’s website. MSF provides medical assistance to people affected by conflict, epidemics, disasters, or exclusion from healthcare. Their actions are guided by medical ethics and the principles of impartiality, independence and neutrality. MSF Australia does not receive public institutional funding.
Read the MSF Australia blog series.


