
Earlier this year, Papua New Guinea’s Prime Minister James Marape proposed that polygynous marriage in the country be outlawed by 2030 to protect women. This will be a big shift in family structures and culture. In PNG, polygynous unions are not uncommon. While the majority of women, around 81.2% of women, are in monogamous unions, the other 18.8% are in polygynous unions. One of us, Mambon, showed in a previous article that polygyny, which was once practised mostly in certain regions, is now spreading across the country. In this article, we ask: do women in polygynous marriages have weaker voices than those in monogamous marriages?
Women’s empowerment or their voice is proxied using three standard decision-making variables. These variables are whether a woman has a say in: (1) decisions about her own health care, (2) large household purchases and (3) visits to immediate family and other relatives.
Before answering the question proposed above, we first investigated the broad trends in women’s empowerment in the country’s last national Demographic and Health Survey. We observed three. First, women’s participation in household decision-making increases with age, education and paid employment. Participation in all three decisions rises from 45.2% among women aged 15 to 19 to 67.9% among women aged 45 to 49. For education, women with no education have lower participation in all three decisions, at 55.3%, while women with higher education record 71.5%. In paid employment, women employed for cash have the highest participation in all three decisions, at 69.5%, compared with 59.3% among women who are not employed.
Second, empowerment strongly varies across residences, region and provinces. Urban women are rather more likely than rural women to participate in all three decisions, with 64.8% of urban women participating compared with 61.2% of rural women. Women in the Islands region record the highest participation in all three decisions, at 69.4%, while women in the Highlands record the lowest, at 55.1%. Provinces such as Madang, Gulf, East Sepik, Manus, New Ireland and East New Britain show relatively high levels of women’s participation in all three decisions. In contrast, Southern Highlands, Jiwaka and West New Britain record some of the lowest levels.
Third, household status matters, but empowerment is not determined by wealth alone. Women with more living children tend to report higher participation in decision-making. For example, women with no children report 52.7% participation in all three decisions, while women with five or more children report 65.2%. An implication is that greater household responsibility and status come with motherhood. However, women in the lowest wealth quintile report 61.6% participation in all three decisions, while women in the highest quintile also report 61.6%. Being in a wealthy household does not necessarily mean there are equal power dynamics between the couples.
We next compared women in monogamous and polygynous marriages to see how likely they were to have a say in the three decision-making areas. To do this, we analysed data from a nationally representative sample of 9,625 married women aged 15 to 49 from the most recent Demographic and Health Survey, using statistical methods that ensure the results reflect the broader population.
We estimated separate models for each of these decision-making variables as our outcome variables, including whether the woman participated in all three decisions. For these four outcome variables, the key explanatory variable was whether the woman was in a polygynous union. The models controlled for age, education, employment, number of living children, household wealth, rural-urban residence, region and acceptance of wife beating.
Our adjusted results show that the association between polygyny and a woman’s voice remains negative across all four outcomes, although the strength of the relationship differs by decision type (Figure 1). The estimated effect is small for own health care, at about 0.6 percentage points lower, and larger for large household purchases, at about 2.9 percentage points lower. The association is stronger for visits to relatives, where women in polygynous unions are about 3.2 percentage points less likely to have a say, and strongest for the combined measure: women in polygynous unions are about 5.2 percentage points less likely to participate in all three household decisions. While the estimates for own health care and large purchases are less precise, estimates for visits to relatives and all three decisions are statistically meaningful. (See table 3 of our regression results.)
Figure 1: Average marginal effect of polygyny on women’s voice
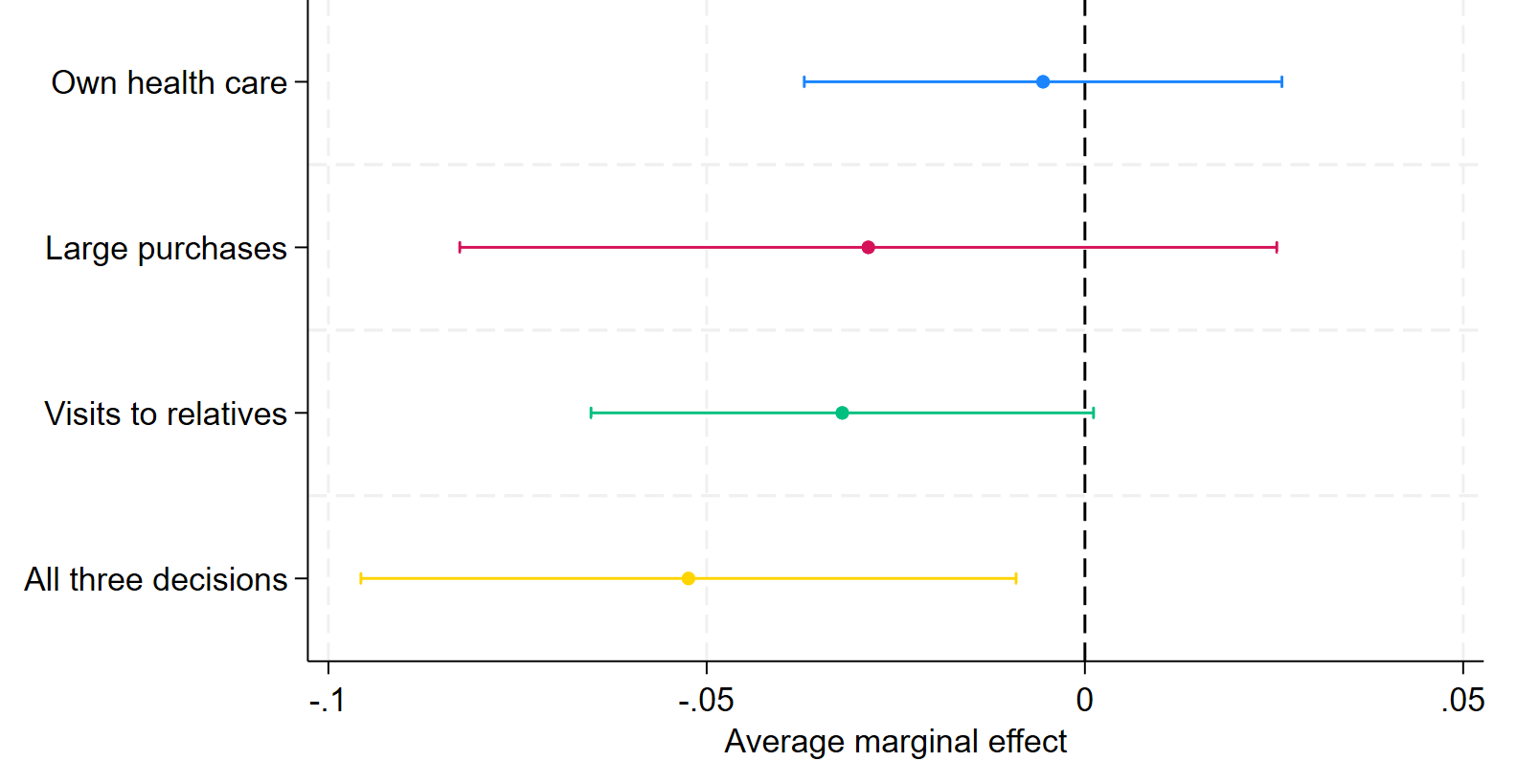
Source: Demographic and Health Survey 2016-18, adjusted survey-weighted logit models.
Our findings are consistent with international evidence, which shows that women in polygynous unions often report lower household decision-making autonomy. For instance, in Mauritania, Florence Anfaara and colleagues found that, after accounting for socio-economic and demographic factors, women in polygamous unions’ odds of participating in decisions about their own health and large household purchases were each 35% lower, while their odds of participating in decisions about visiting family or relatives were 28% lower compared to those in monogamous marriages.
In sum, marriage structure matters for women’s empowerment in PNG. Women in polygynous unions appear to have a weaker voice in household decision-making. Our estimates have shown that polygyny is a risk factor for women’s voice. And as shown by general trends, encouraging women to delay marriages, supporting them to complete their education and engaging them in paid work are potentially protective factors.





