
On 6 March The Weekend Australian reported that Queensland will fast-track the AstraZeneca vaccine into the Torres Strait, as the COVID-19 outbreak in Papua New Guinea worsens and Australian authorities grow increasingly concerned about the porous northern border (see also here).
Through February and early March, reported COVID-19 cases in PNG increased by 73 percent, from 865 to 1,493. The death toll increased from nine to 16. By global standards these numbers are small, though by Pacific standards they are large. However, within PNG the rate of testing has been low and it is likely that many cases have gone unreported. The parlous state of PNG’s health facilities suggests that the country may be already approaching a limit to possible containment (here, here and here). There are concerns, moreover, that PNG could export the virus eastwards to other Pacific nations and that the outbreak may have geopolitical implications.
It is in this context that Queensland is acting on behalf of its own citizens, both those on islands like Boigu and Saibai that are less than 10 km from PNG’s Western Province, and those on the mainland to the south. As Australians, the people of Boigu and Saibai have potential access to material conditions and services like those available to residents of the mainland. The privileged lifestyles of the latter, however, are beyond the experience and the reach of their Western Province neighbours who ‘endure a near-total failure of governance and service delivery’.
Queensland’s concern is valid. The response, however, may be misguided.
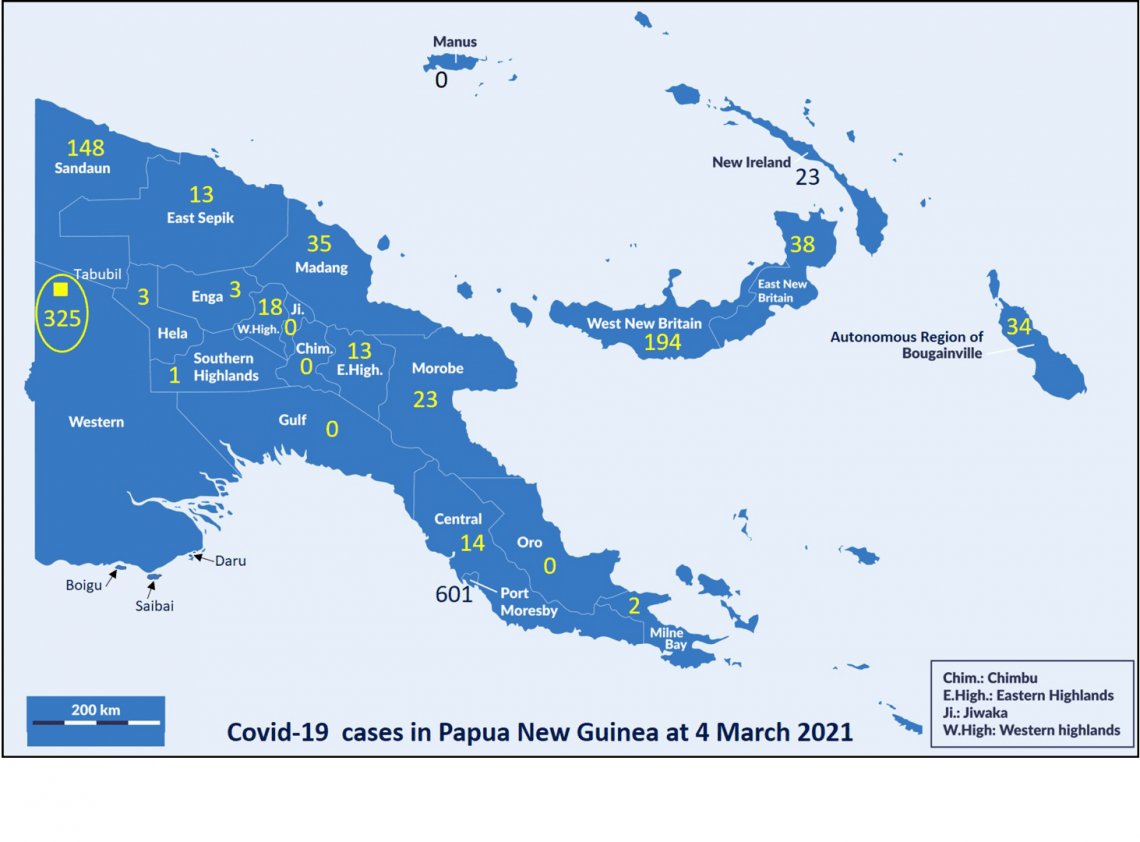
The map at the head of this article shows the distribution of reported COVID-19 cases in PNG at 4 March 2021. Cases have been reported from the National Capital District (Port Moresby and surrounds) and 16 of the other 21 provinces. The distribution is very uneven. Three provinces – National Capital District, Western Province and West Sepik – have contributed 479 (76 percent) of the 628 new cases recorded in the past five weeks. West Sepik jumped from a total of two to 146 cases in those weeks, with outbreaks among hospital staff and at correction centres.
For Queensland, however, Western Province is its nearest neighbour and must be focal. With 325 reported cases at 4 March, this province is second only to National Capital District in its tally of COVID-19 cases. But, as indicated on the map, all of those cases were recorded from the north of the province, with all but four from the Ok Tedi mining town of Tabubil and some of its surrounding villages.
Present infection statistics provide no direct evidence that coastal communities of Western Province pose a COVID-19 threat to Australia. Far from it. None of the COVID-19 cases in that province has been detected from coastal communities close to Australia; to the contrary, they have all been detected more than 350 km north of the northern limit of Australia.
Gulf Province, encompassing coastal communities to the immediate east of Western Province, has not yet recorded any cases of COVID-19. The current threat to Queensland comes from the north of Western Province, and it comes from the well-off rather than from the desperately poor. In early March, five cases detected in the north Queensland city of Cairns were Ok Tedi workers who had arrived by charter flight from Tabubil. They were not the first COVID-carrying, fly-in fly-out, passengers to come from PNG.
Ok Tedi Mining Ltd. has been monitoring its work force since August last year. Queensland can test international arrivals and quarantine them as needed. Therefore, a potential threat from that quarter can, presumably, be managed.
But what should happen in the south where, at present, there is no evidence of imminent threat but where there is always the potential for a threat to emerge? It is the potential that should be managed. But that potential is not located on Australian islands in Torres Strait. It is located nearby on the mainland of PNG. Health facilities in the south of Western Province are in a disgraceful state. Cases of TB are already at a shocking level. If COVID-19 does get a hold here then, irrespective of the dedication of medical staff, there is no infrastructure and there are no resources to hold it at bay.
This is where Queensland, and Australia, should prioritise effort. Targeting the urgent health needs of people in the south of Western Province would allow simultaneous, and much needed, monitoring of COVID-19. It would show, first, whether there was actually a need for greater intervention both within and beyond the south of Western Province and, subsequently, direct attention to modes of intervention that did not have the appearance of constructing a wall of immune bodies to guard the lives of southerners. The reciprocity implicit in serving one’s own needs and interests through contributing positively to the needs of others would resonate well with local understandings in PNG.
The present proposal to vaccinate Australian citizens who live close to PNG will be, without doubt, beneficial to those people. It might be also imagined as safeguarding people who live in Cairns or Brisbane, though it is far from necessary for this. It will not, however, do anything at all toward improving the health of, or enhancing relations with, Papua New Guineans who live just a short boat trip away. These are men, women and children who have none of the advantages that sometimes accrue to their friends and relations who, by the accident of a line drawn on a map, became citizens of a different country.



Hi Monica and Peter, I am surprised by the high count in West New Britain. No mining camps there, but there are logging companies and of course oil palm.
Hi Patrick
WNB cases started to take off in late November and through December 2020. By end of January 2021 recorded tally was 177. To that time, majority of cases were from Talasea district with, I suspect, an oil palm fly-in-fly-out workers’ link. Then, as with Bougainville, cross-province meetings [in person, not via Zoom] to discuss emerging Covid-19 problems and solutions became initiating and spreading events. At 14 March WNB count is 195.
Oil Palm workers on New Britain Island do NOT fly in fly out. They are nationals who live and work on estates.
Thanks, Netta. Perhaps there was a semantic difficulty. I always think of CEOs, senior executives and scientifically-trained employees of companies as ‘workers’. When I checked the web site for New Britain Oil Palm it seemed that many on the company’s work force were not ‘born and bred’ West New Britainers. Are any of them ‘mainlanders’ who fly in and fly out? If I’ve got it wrong, thanks for the correction. But as someone with strong ties to West New Britain and oil palm it would be great if you could help us understand how Covid-19 took off in the Talasea district.
No worries Peter. Yes, the higher up levels of NBPOL and Hargy and are expats but we all live onsite and are not fly in fly out of the province. In fact these companies both put strict travel bans on all employees for the balance of last year (I was forced to leave the country as a “non-essential employee” for 8 months). All other spouses of company executives left a month before I did in April 2020 and they remain outside the country. I was able to return due to my employment. Those employees who have travelled have been subject to a double quarantine regime whereby they quarantine on return to the country in POM and then again on return to the island. This did not happen all the time but once numbers began to increase these measures were reinstated by the companies.
The labourers are housed on site on plantations. There is a certain amount of “cultural” (in the event of family deaths) migration which occurs with workers travelling back to home provinces at these times. However, this is not a huge amount of traffic.
The largest traffic on and off the island is due to government employees and staff/owners of larger (due to higher disposable incomes) local businesses travelling to and from POM and Lae etc. Planes are Max loaded/overloaded with people not wearing masks correctly if at all. These are the biggest issues to my mind.
There are significant issues with testing: correct procedures testing being followed; delay of 30 +/- days for results; mobility of population affects the re-contacting of those who may test positive; mobile phone coverage very poor and not widely held (people do not always have credit), no isolation once testing has been done, severe limitations around contact tracing…these issues go on. I was tested during the lockdown in early January due to showing mild unspecific symptoms. The health worker who took the test on the side of the road did not wear gloves or PPE beyond a surgical mask, inadvertently touched the tip of the swab after withdrawing from my nose; advised me they would phone results through within 5-7 days which never happened. I waited 8 days, quarantining myself by not leaving my home, before giving up. My symptoms had subsided and I was feeling well for most of that time.
You would be aware of the huge geographical, language, social and cultural limitations that exist in the country. These are exacerbated on the island. I recommend you establish contact and dialogue with Jack O’Shea of Australian Doctors International (currently in quarantine in Cairns having returned to Australia for a short period of time) who has been based on the island since the end of 2019. Jack would be a highly credible source of information with valuable insights into the issues faced on the island in the area of health delivery gained from his efforts to roll out obstetrics and other programs in isolated areas of the island.
I am conscious my observations are anecdotal only, thus with little credibility. I have huge empathy and respect for these people. My husband runs a Palm oil plantation for NBPOL and we have around 1500 who live in company housing on the estate. We constantly struggle to provide some semblance of a covid safe environment, however due to overcrowded accommodation, betel nut chewing and spitting, the cultural practice of sharing drinks/food freely which signifies respect and friendship between themselves, lack of ability to adhere to strict hygiene practices required when infection risks are heightened, use of PMVs to go to town (always overcrowded with no-one wearing masks, attendance at religious rallies held in town around the shopping and market areas…we are failing these people.
I do hope you find some use in my writings and I do urge you to make contact with Jack O’Shea. Further, should you ever come to New Britain Island I extend an invitation to meet and talk further. I am not sure if you have either been to, or heard of, Walindi resort: we are located very close by.
Thank you for this article, which adds nuance to the COVID picture in PNG without taking anything away from the urgency of the need for Australia to step up.
The map is especially useful as a guide, but it’s worth noting that the parlous state of the health system in the south of Western Province makes it quite possible that the virus is present there, undetected. Of course this only strengthens your argument for a cross-border approach!
This article and Jonathan Pryke’s piece in The Australian and on Lowy today both call for Australia to step in urgently – and we should. But this is clearly a situation that would benefit from a larger, more coordinated approach than we can offer on our own. What might be achieved through cooperation with India (who are donating vaccine), Indonesia, the US and even China? I’ve tried and failed to find a global risk analysis for COVID management but even if the risk to the Torres Strait is minimal, the impacts of an uncontrolled outbreak within PNG, and the risk of transmission east to the Pacific islands marks PNG as a critical piece of the puzzle. A concerted international effort might also be effective in countering the low levels of concern and growing vaccine hesitancy which seem to be widespread in the country.
From Peter Dwyer & Monica Minnegal
Thanks James. We agree, there is a high probability that the virus is already working its way through communities in the south of Western Province. But the desirability of a cross-border approach has not just emerged. The Australian island of Boigu is 205 km east-south-east from Merauke in the Indonesian province of Papua or 120 km east of the PNG-Indonesian border. That’s a lot closer to Australia than either the Ok Tedi mining town of Tabubil or Port Moresby. In late November 2020, the Merauke catchment had recorded 188 cases of Covid-19. On subsequent trends in Papua as a whole, the count now may well exceed 400. Official bans on international travel did not effectively curtail Indonesia-PNG border crossing by either land or sea through 2020. Some traders from Indonesia reached Gulf Province in this period. It is possible, even likely, that the virus lurks in the south of Western Province and it is therefore desirable that, on behalf of PNG, Australia checks this out. But we have known for many months of a real, not imagined, risk from the west yet have not acted to protect Torres Strait islanders from that. A little odd!