
This is the second post in a two-part series. In the first post the context of PNG’s free health care policy was provided and the findings of the PEPE survey on health financing were summarised.
Implications for PNG’s free primary health care policy
PEPE survey findings offer insights into how a free primary health care policy could impact the finances available to health facilities in PNG. The implications of the policy will differ across provinces due to the variation in the fees collected by facilities for consultations and drugs, as well as the number of patient visits. In order to identify key implementation issues that may have an impact on the policy, several important challenges are highlighted.
Whether the budgeted subsidy payments allocated under the policy will be sufficient to offset the user fees that health facilities normally collect needs to be considered. Using survey data on user fees collected by health facility type, total annual fees raised were estimated as being close to K12 million. This figure is slightly higher than the total subsidy allocations made through the free primary health care policy in 2014, which indicates that total subsidy payments maybe insufficient to offset fees. However, the more relevant issue is how subsidy payments will be allocated across provinces. Due to the large disparities in the fees collected, if subsidy payments are allocated evenly, some provinces may receive too much funding, while others will not receive enough, which will have an impact on the ability of health clinics to deliver services.
A practical example of funding shortfalls resulting from the policy was presented by the Head Administrator of the Kudjip Nazarene Hospital in the newly formed Jiwaka Province at the recent PEPE budget forum. This high-performing rural hospital provides primary and secondary health care and is described as a successful public-private partnership between the church and the state, but it would be unable to both comply with the policy and deliver the same quality of care as it currently provides.
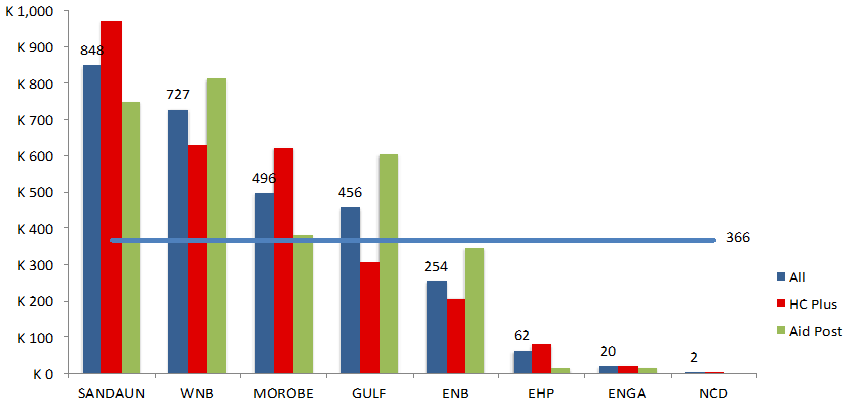
There is also a need to find a viable and cost effective funding mechanism for getting subsidy payments to health workers at the facility-level. The magnitude of this challenge should not be underestimated given the high cost of accessing financial services across PNG. Every health facility would need to be reached with funding to make the policy work, which is difficult considering that about two-thirds of health facilities are aid posts, which are normally located in rural and remote areas. The PEPE survey collected data on the total costs for health workers to access banking services and return to their posts. The chart below shows that the average cost is more than K350, and that there is enormous variation across provinces.
Cost in Kina to collect pay and return to aid post: all expenses
 Another potential challenge is that of distributing subsidy payments to health facilities at regular intervals. Survey data indicates that many health facilities collect small amounts of fees, often. Having some funding available all the time seems to be important for meeting basic costs, such as paying for fuel to collect medical supplies or maintain basic utilities. Keeping the same arrangements in place under the new policy may be more difficult for rural health facilities that normally collect less revenue from fees and are more costly to reach. Abolishing the user fees that are important for paying the costs of delivering essential services comes with significant risks. If health facilities have to forego charging fees and rely on a convoluted financing system, they may be unable to deliver the same quality of service.
Another potential challenge is that of distributing subsidy payments to health facilities at regular intervals. Survey data indicates that many health facilities collect small amounts of fees, often. Having some funding available all the time seems to be important for meeting basic costs, such as paying for fuel to collect medical supplies or maintain basic utilities. Keeping the same arrangements in place under the new policy may be more difficult for rural health facilities that normally collect less revenue from fees and are more costly to reach. Abolishing the user fees that are important for paying the costs of delivering essential services comes with significant risks. If health facilities have to forego charging fees and rely on a convoluted financing system, they may be unable to deliver the same quality of service.
Simply increasing subsidy payments for health facilities in a similar manner to schools under the tuition fee-free policy is unlikely to be an appropriate short-term solution. School survey data indicates that subsidy payments reach bank accounts, although funding for the tuition fee-free policy is much higher than the free primary health care subsidy payments. Schools are also much better positioned to manage higher levels of funding through established governance mechanisms, including a Board of Management. Most health facilities do not have the same structure to effectively administer similar levels of funding. Direct financing to schools offers some insights into possible approaches that health facilities might use to establish management structures capable of absorbing more funding.
Conclusion
The free primary health care policy will have significant implications for services delivered at health facilities across PNG. PEPE health survey data suggests that user fees have become the most widely available, easily accessible and reliable source of funding for health facilities in the delivery of front-line services.
While the intention of the free primary health care policy is to improve access to services, the implementation risks may weaken, rather than strengthen, the health system. PEPE survey findings suggest that health facilities need more reliable financial support for front-line service delivery before they can move away from charging user fees. The importance of establishing a feasible mechanism for financing health facilities cannot be understated, and is more complex than simply putting funds into bank accounts. Access to cash, especially for remote facilities, is important for paying basic operational costs.
Moving slowly and learning by trialling approaches to implementation that already work might be the best way forward from a technical standpoint. However, a steady approach may conflict with political pressures intent on immediately implementing the free primary health care policy across PNG. This could lead to either non-compliance or poorer quality services delivered, neither of which would result in better health services delivered to the people of PNG.
The complete discussion paper, ‘Financing PNG’s free primary health care policy: user fees, funding and performance’, can be accessed here.
Colin Wiltshire is the Devpolicy Program Manager for the PNG Promoting Effective Public Expenditure Project. He is also undertaking a PhD in the State, Society and Governance in Melanesia (SSGM) Program at ANU. Andrew Anton Mako is a Research Fellow at PNG’s National Research Institute and a Research Associate of the Development Policy Centre.





