
 Providing free primary health care is a key policy priority of the current Papua New Guinea Government. The Prime Minister, Peter O’Neill, has made reference to his government’s aspirations of ‘saving mothers the one and two kina’ that it can cost them and their children to visit health facilities across the country. The introduction of a free health care policy can be perplexing in the PNG context, considering primary health services should already be provided free of charge. Rather than enforcing existing laws and policies, the central premise of the new policy is to subsidise health facilities with direct payments in place of fees they would have collected from patients. While such an arrangement may seem sound in theory, the PNG Government has long struggled to find practical solutions for funding health facilities to deliver services.
Providing free primary health care is a key policy priority of the current Papua New Guinea Government. The Prime Minister, Peter O’Neill, has made reference to his government’s aspirations of ‘saving mothers the one and two kina’ that it can cost them and their children to visit health facilities across the country. The introduction of a free health care policy can be perplexing in the PNG context, considering primary health services should already be provided free of charge. Rather than enforcing existing laws and policies, the central premise of the new policy is to subsidise health facilities with direct payments in place of fees they would have collected from patients. While such an arrangement may seem sound in theory, the PNG Government has long struggled to find practical solutions for funding health facilities to deliver services.
The free health policy came into effect on 24 February, 2014 but has been met with apprehension from those tasked with its implementation. Health service providers and officials have expressed deep concerns about the implementation of the policy. Hospital managers have said that it could ‘cost people their lives’ calling it a ‘politicians’ policy’, while one prominent public official (who will remain nameless) has publically stated that health services are already weak in PNG and this free health policy could collapse the system.
Such negative criticism of a free health policy may appear harsh, as committing to provide services free of charge sounds like a positive development. Costs can be a barrier to access, especially for poorer communities, and removing fees could improve accessibility to services. However, the criticism is not levelled at the concept of providing free health services but the consequences of implementing the policy in the context of a poorly functioning health system. User fees are often the only source of revenue for health facilities that keep them operational and charges are normally exempt for those who cannot afford to pay.
Survey findings from the Promoting Effective Public Expenditure (PEPE) Project suggest that health officials have good reason to suspect that the immediate implementation of the policy could well impact the ability of health facilities to deliver services. In September 2013, the PEPE project presented the preliminary findings of health survey data labelled ‘PNG’s lost decade’, which compared our results to a similar study from 2002 to show that health services had generally declined over the last 10 years. Significant weaknesses across the health system were revealed, such as deteriorated infrastructure, health workers not at their posts and shortages of available drugs despite large increases in funding to the sector over the same period. One key finding was the reliance on user fees for health facilities to deliver front-line services, as a common, reliable funding source was not evident from the survey data.
PNG’s National Department of Health invited PEPE project researchers to present a discussion paper on the challenges to implementing the free health policy at the 2014 National Health Conference in Port Moresby. This was an excellent opportunity to disseminate research findings to the senior health officials from across PNG that are charged with implementing this controversial policy.
This two-part blog series provides a summary of the key findings presented in the discussion paper, ‘Financing PNG’s free primary health care policy: user fees, funding and performance’. This first post gives an overview of the survey findings related to finances available at health facilities, and the second will discuss the challenges to implementing the free primary health care policy. A full-version of the paper distributed at the conference can be accessed here.
PEPE survey findings on health financing
A key focus of PEPE health surveys was to assess how health facilities receive financial support to deliver basic services. One of the two health expenditure reforms tracked through the survey was the health function grant, which should provide funding for health facility operations (see this recent Devpolicy blog post from Alan Cairns on rural health funding). The PEPE health surveys collected data on all revenue raised at the health facility through user fees, funding received through budgets or as direct payments. This included the administered (or in-kind) support delivered to health facilities in the form of goods and services from funding providers.
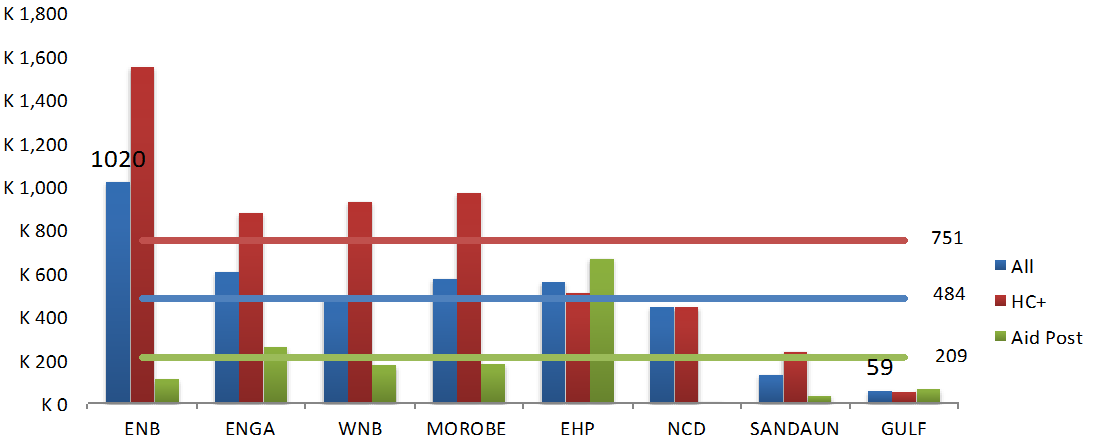
Survey results confirmed that the majority of health facilities charge their patients fees for consultations and drugs. However, the various types of services offered and drugs administered usually result in different costs across provinces. Therefore, total fees raised by health facilities are widely variable as some provinces already provided free health services at the time of the survey, while others actively encourage their facilities to charge fees. For instance, the average health facility in East New Britain collects more than K1,000 a month from fees, whereas health facilities in Gulf Province raise just K59 a month, as seen in the graph below. Church-run health facilities are more likely to charge for services provided and ask a higher fee than state-run facilities.
Average monthly user fees raised at health facilities (Kina)
 Fees raised by health facilities are important for funding operational expenses and delivering front-line services. Patients that cannot afford fees are still able to receive treatment in most circumstances. Fees are usually exempt, or patients are allowed to pay according to their ability or make an in-kind contribution. However, as the law has always stated, fees should not be charged for the services provided. Instead, health facilities should be adequately funded through government or church health providers to meet basic service delivery requirements.
Fees raised by health facilities are important for funding operational expenses and delivering front-line services. Patients that cannot afford fees are still able to receive treatment in most circumstances. Fees are usually exempt, or patients are allowed to pay according to their ability or make an in-kind contribution. However, as the law has always stated, fees should not be charged for the services provided. Instead, health facilities should be adequately funded through government or church health providers to meet basic service delivery requirements.
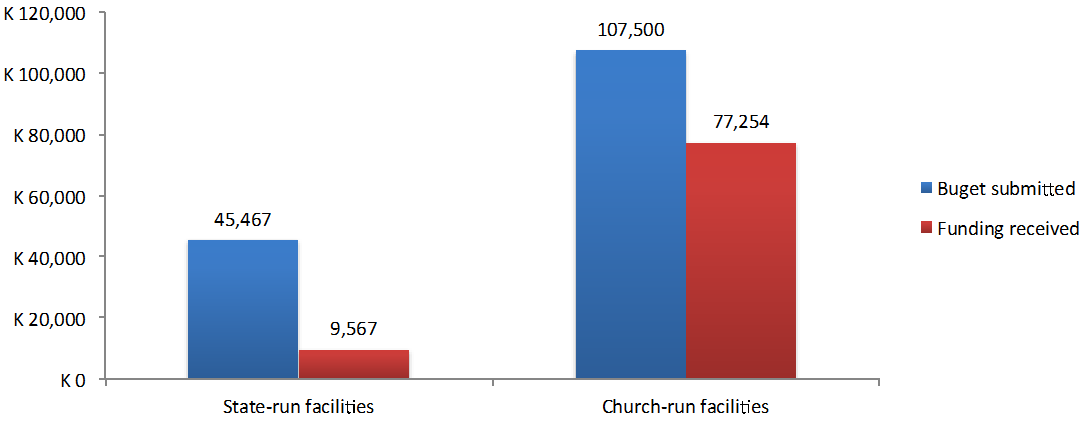
There are widespread disparities in how health facilities are financed across provinces, particularly between state and church-run providers. Most health facilities do not submit budgets or plans in anticipation of receiving funding. Of those that do submit budgets, less than half receive any funding as a result and the average value of funding received is generally much lower than has been budgeted. Some health facilities receive direct funding without preparing a budget and the average funding received was much higher than for those that prepare budgets. Church-run health facilities are much more likely to receive funding from budgets and the amounts are higher than state-run facilities, as detailed in the chart below. Health facilities that receive their own funding to deliver services, either from budgets or as direct payments, was lower than expected from the survey results.
Budgets submitted and funding received by health facilities (church vs state)
 There have been large increases in national budget allocations in the last decade intended to assist health facilities with their basic operations. However, much of this funding is not directed at the facility-level to be managed by the health workers who deliver services. Rather, the most common ways in which health facilities receive support for delivering services is through administered assistance from funding providers. This means either supplies or materials are purchased on behalf of health clinics or support is provided for health activities and programs. While administered support is the most common form of assistance, it does not mean the support provided is consistent or sufficient to meet minimum health standards.
There have been large increases in national budget allocations in the last decade intended to assist health facilities with their basic operations. However, much of this funding is not directed at the facility-level to be managed by the health workers who deliver services. Rather, the most common ways in which health facilities receive support for delivering services is through administered assistance from funding providers. This means either supplies or materials are purchased on behalf of health clinics or support is provided for health activities and programs. While administered support is the most common form of assistance, it does not mean the support provided is consistent or sufficient to meet minimum health standards.
This is the first of a two-part series. Read Part 2 here.
Colin Wiltshire is the Devpolicy Program Manager for the PNG Promoting Effective Public Expenditure Project. He is also undertaking a PhD in the State, Society and Governance in Melanesia (SSGM) Program at ANU. Andrew Anton Mako is a Research Fellow at PNG’s National Research Institute and a Research Associate of the Development Policy Centre.





